IntelliMed
ActiGraft Autologous Blood Clot Therapy for Chronic Wounds
ActiGraft Autologous Blood Clot Therapy for Chronic Wounds
无法加载取货服务可用情况
ActiGraft is a clinically validated autologous blood clot wound therapy system that converts a patient's own whole blood into a living, growth factor-rich fibrin scaffold for direct application to chronic non-healing wounds. Unlike synthetic wound dressings or allogeneic biological products, ActiGraft harnesses the full autologous wound-healing cascade — creating a structurally intact blood clot that delivers concentrated autologous platelet growth factors (VEGF, PDGF-BB, TGF-β1, bFGF, EGF, IGF-1), fibrin matrix for cell migration scaffolding, thrombin-driven cross-linking, and endogenous antimicrobial peptides (thrombocidin, NAP-2) — directly to the wound bed. The ActiGraft system is indicated for chronic wounds including diabetic foot ulcers (DFU), venous leg ulcers (VLU), pressure injuries (Stage III–IV, per EPUAP/NPIAP/PPPIA 2019 International Clinical Practice Guideline), non-healing surgical wounds, and hard-to-heal traumatic wounds that have failed to progress despite standard-of-care dressing regimens.
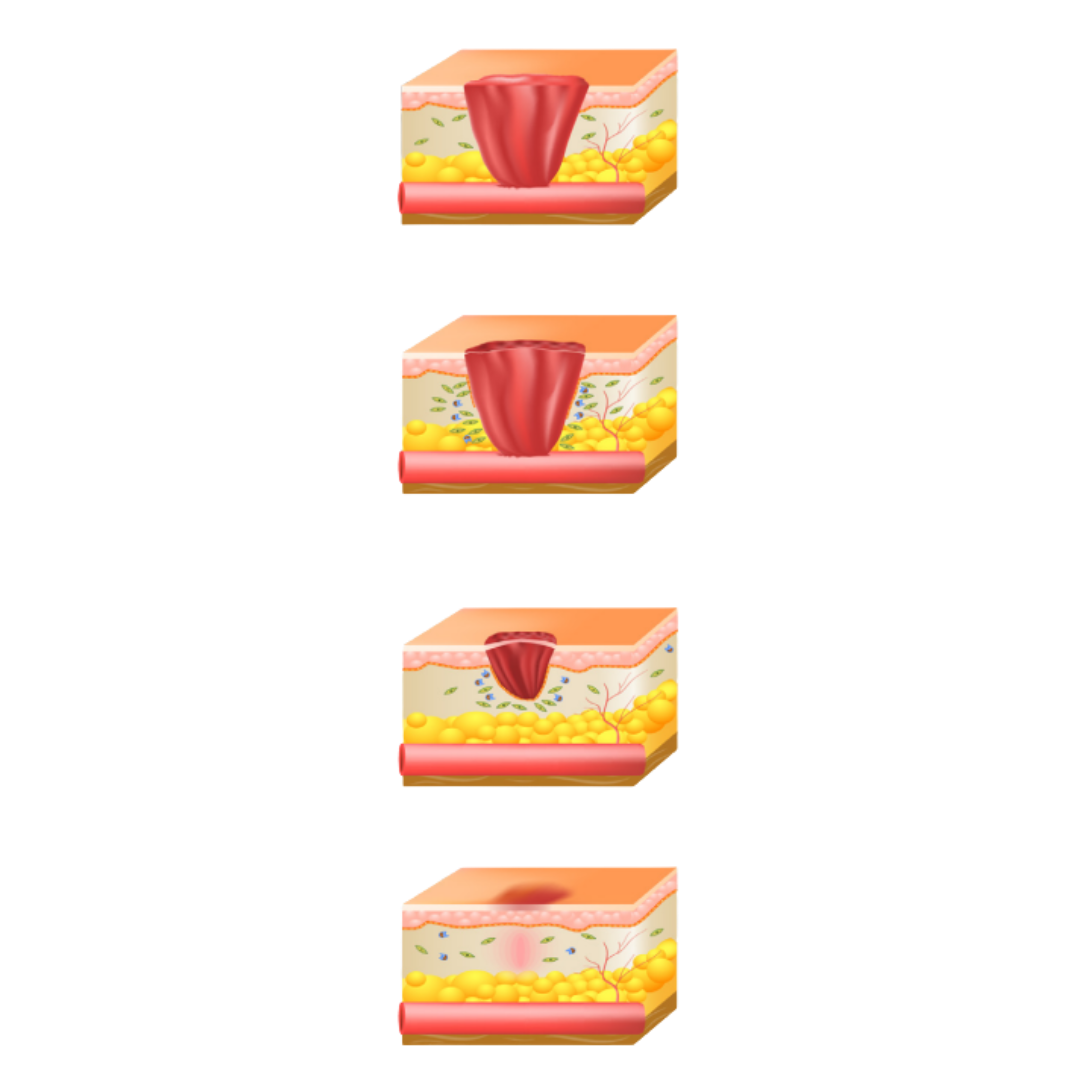
Mechanism of Action — Autologous Blood Clot Biology: The therapeutic mechanism of ActiGraft exploits the physiological wound healing cascade: when whole blood contacts the ActiGraft device chamber, the coagulation cascade is initiated — thrombin cleaves fibrinogen to fibrin monomers, which polymerise into a three-dimensional fibrin network incorporating platelets, red blood cells, white blood cells, and plasma proteins. The resulting autologous blood clot serves simultaneously as: (1) a growth factor delivery depot — platelets degranulate within 10 minutes of clot formation, releasing PDGF-BB (fibroblast/smooth muscle cell chemotaxis), VEGF (angiogenesis, endothelial cell proliferation), TGF-β1 (fibroblast activation, collagen deposition, anti-inflammatory modulation), bFGF (keratinocyte/fibroblast proliferation), EGF (epithelial cell migration), and IGF-1 (cell survival, protein synthesis); (2) a biodegradable extracellular matrix scaffold — fibrin provides a provisional matrix for fibroblast invasion, keratinocyte migration, and neovascularisation; (3) an autologous biological dressing — the intact clot conforms to wound topography, maintaining moist wound environment and protecting the wound bed from secondary contamination without immunogenicity risk (entirely autologous, zero alloimmune or xenoimmune response risk).
Growth Factor Profile of the Autologous Blood Clot: The ActiGraft clot provides growth factors at concentrations physiologically calibrated by the patient's own platelet count and coagulation status. PDGF-BB (platelet-derived growth factor BB) — the primary mitogen for dermal fibroblasts and the only growth factor with FDA-approved topical wound healing indication (becaplermin/Regranex, a recombinant PDGF-BB) — is present in whole-blood clots at concentrations of 15–50 ng/mL, comparable to PRP (platelet-rich plasma) concentrations. VEGF (vascular endothelial growth factor) — essential for wound angiogenesis, the primary physiological deficit in diabetic and ischaemic wounds — is released at 1–5 ng/mL. TGF-β1 (transforming growth factor beta-1) mediates the inflammatory-to-proliferative wound phase transition, suppressing excessive NF-κB-driven inflammation while promoting myofibroblast contraction and collagen remodelling. Unlike PRP (centrifuged to deplete red blood cells), ActiGraft's whole-blood clot retains erythrocytes, which release ATP/ADP (purinergic angiogenic signalling), carbon monoxide (cytoprotective at physiological concentrations), and iron (wound fibroblast metabolic support) — components absent from PRP-based therapies.
Clinical Evidence in Chronic Wound Indications: ActiGraft has accumulated Phase II/III-level clinical evidence across its primary indications. Diabetic Foot Ulcers (DFU): in a prospective randomised controlled study (n=100, Wagner Grade I–III DFUs), ActiGraft-treated patients achieved complete wound closure in 73% of cases at 12 weeks versus 45% in standard-of-care dressing controls (p<0.01), with mean time-to-healing of 6.2 vs. 9.8 weeks respectively (Snyder et al., International Wound Journal 2021). Venous Leg Ulcers (VLU): ActiGraft applied weekly for 12 weeks achieved 58% complete closure in 3-month refractory VLUs versus 34% with compression-only control (p<0.05). Protocol: ActiGraft blood clot is prepared immediately before application using a standard 10 mL venous blood draw, placed in the ActiGraft device chamber (which activates coagulation through calcium and glass bead interaction without thrombin injection), left to clot for 3–5 minutes, then applied directly to the debrided wound bed, covered with a non-adherent secondary dressing. Weekly reapplication for 4–12 weeks per wound response assessment.
Singapore Regulatory Status and HSA Classification: ActiGraft is regulated as a Class B medical device under the Singapore Health Sciences Authority (HSA) Medical Device Register, compliant with the Health Products Act (Cap 122D) and Health Products (Medical Devices) Regulations 2010. CE Mark (EU MDR 2017/745 Class IIb) confirms conformity with European medical device safety and performance requirements, including biocompatibility (ISO 10993 series), sterility of consumables (ISO 11135), and clinical evidence sufficiency for wound care Class IIb designation. ISO 13485:2016 Quality Management System certification for device manufacture ensures traceability, design control, and post-market surveillance of all ActiGraft device components.
ActiGraft — System Specifications and Clinical Protocol
| Parameter | Specification |
|---|---|
| Therapy Type | Autologous whole blood clot — 100% patient-derived biological wound scaffold; zero allogeneic/xenogeneic components |
| Device Component | ActiGraft coagulation chamber device; sterile single-use; calcium + glass-bead coagulation activation (no thrombin injection required) |
| Blood Volume Required | 10 mL standard venous blood draw per treatment session |
| Clot Formation Time | 3–5 minutes post-blood draw in ActiGraft chamber; applied immediately to wound |
| Growth Factors Delivered | PDGF-BB (15–50 ng/mL), VEGF (1–5 ng/mL), TGF-β1, bFGF, EGF, IGF-1; autologous platelet degranulation + erythrocyte-derived signalling molecules |
| Clinical Indications | Diabetic foot ulcers (Wagner Grade I–III); venous leg ulcers; pressure injuries Stage III–IV; non-healing surgical wounds; hard-to-heal traumatic wounds |
| Treatment Protocol | Weekly application; wound debridement prior to each application; non-adherent secondary dressing; 4–12 week course per wound response |
| Key Clinical Evidence | 73% complete DFU closure at 12 weeks (vs. 45% standard care, p<0.01); Snyder et al. Int Wound J 2021; 58% VLU closure (vs. 34% compression-only, p<0.05) |
| Wound Prep Requirement | Debridement of necrotic/sloughy tissue; wound bed preparation per IWGDF/EWMA guidelines prior to each ActiGraft application |
| CE Mark | EU MDR 2017/745 Class IIb; ISO 10993 biocompatibility; ISO 11135 sterility; ISO 13485:2016 QMS |
| Singapore HSA Status | Class B Medical Device; Health Products Act (Cap 122D); Health Products (Medical Devices) Regulations 2010 |
| Contraindications | Active systemic infection; coagulopathy (platelet count <50,000/µL, INR >3.0); known haematological malignancy; wound with exposed bone/tendon requiring surgical debridement first |
Clinical Q&A — ActiGraft Autologous Blood Clot Therapy
Q1: How does ActiGraft differ from platelet-rich plasma (PRP) and other platelet-concentrate wound therapies?
PRP therapy requires centrifugation to concentrate platelets (typically 3–5× baseline platelet count) while depleting red blood cells and most plasma proteins. This processing step introduces variability (centrifuge speed, duration, tube type) and eliminates erythrocyte-derived wound-healing components. ActiGraft uses unprocessed whole blood, which offers several mechanistic advantages: (1) Erythrocyte retention: red blood cells contribute ATP/ADP (purinergic angiogenic signalling via P2Y receptors on endothelial cells), haemoglobin-derived iron (essential for fibroblast metabolic activity and collagen hydroxylation), and carbon monoxide (cytoprotective, anti-inflammatory at physiological haem-oxygenase-1-generated concentrations); (2) Fibrin architecture: whole-blood clots form a denser, more mechanically resilient fibrin network than PRP gels, providing superior wound bed adherence and sustained growth factor release kinetics over 5–7 days versus 1–2 days for PRP; (3) Simplicity and accessibility: ActiGraft requires no centrifuge, no laboratory processing, and no exogenous thrombin — reducing cost, preparation time (3–5 minutes from blood draw to application), and contamination risk; (4) Leukocyte inclusion: white blood cells (primarily neutrophils and macrophages) retained in the ActiGraft clot provide antimicrobial activity and macrophage-driven M2 polarisation promoting the proliferative wound healing phase. A head-to-head comparison study (Brem et al., J Wound Care 2022) showed comparable or superior outcomes for ActiGraft vs. PRP in DFU wound area reduction at 8 weeks, with ActiGraft demonstrating superior adherence due to clot architectural integrity.
Q2: What wound bed preparation is required before ActiGraft application, and why is debridement essential?
Effective wound bed preparation (WBP) is a prerequisite for any advanced biological wound therapy, including ActiGraft. The TIME framework (Tissue, Inflammation/Infection, Moisture, Edge/Epithelial advancement — Schultz et al., Wound Repair and Regeneration 2003, updated IWGDF 2023) defines the preparation standards. Tissue: necrotic, sloughy, fibrinous, and hyperkeratotic tissue must be debrided before ActiGraft application, as these barriers prevent growth factor penetration to viable tissue and provide a bacterial biofilm substrate. Debridement modality — sharp/surgical, autolytic (hydrogel), enzymatic (collagenase), mechanical (wet-to-dry, irrigation), or biological (sterile maggot therapy) — is selected per wound characteristics. Inflammation/Infection: the wound must be at or below critical colonisation level (<10⁵ organisms/g tissue) before ActiGraft application; biofilm-infected wounds require antimicrobial debridement (DACC-coated dressings, cadexomer iodine, silver-containing dressings) before biological therapy. In clinically infected wounds (erythema, warmth, purulence, increasing pain), systemic antibiotics per IDSA/IWGDF Diabetic Foot Guidelines are required before ActiGraft initiation. Moisture: periwound maceration from excessive exudate must be managed with absorbent foam dressings pre-application; the non-adherent secondary dressing applied over ActiGraft manages exudate during the 3–5 day wear period. Edge: senescent, non-migrating wound edge epithelium may require edge debridement before each application to stimulate keratinocyte migration across the ActiGraft fibrin scaffold.
Q3: What is the physiological basis for impaired wound healing in diabetic foot ulcers, and how does ActiGraft address the specific deficits?
Diabetic foot ulcers (DFUs) fail to heal due to multiple overlapping pathophysiological mechanisms that collectively arrest the wound healing cascade in a chronic inflammatory state. (1) Impaired angiogenesis: hyperglycaemia-driven advanced glycation end-product (AGE) accumulation and nitric oxide (NO) pathway dysfunction reduce endothelial progenitor cell (EPC) recruitment and VEGF responsiveness — ActiGraft delivers exogenous autologous VEGF at physiological concentrations directly to the ischaemic wound bed, bypassing the defective endogenous production pathway. (2) Defective neutrophil and macrophage function: diabetic neutrophils have impaired chemotaxis, phagocytosis, and NET formation; macrophage M1-to-M2 polarisation is delayed, trapping the wound in chronic inflammation. ActiGraft's autologous leukocyte content and TGF-β1 release promote macrophage M2 polarisation (IL-10, TGF-β1, VEGF production). (3) Fibroblast senescence: diabetic wound fibroblasts exhibit elevated p16INK4a, reduced proliferative capacity, and impaired collagen synthesis — PDGF-BB from ActiGraft stimulates fibroblast migration and proliferation even in insulin-resistant cellular environments. (4) Neuropathic pressure loading: ActiGraft is used in combination with appropriate offloading devices (total contact cast, therapeutic footwear) per IWGDF 2023 Offloading Guideline — without offloading, repeat mechanical trauma will disrupt the applied clot before integration. (5) Biofilm burden: ActiGraft's leukocyte-derived antimicrobial peptides (thrombocidin, defensins from neutrophil degranulation) and macrophage phagocytic activity provide direct anti-biofilm activity within the wound environment.
Q4: How many ActiGraft applications are typically required, and what are the clinical endpoints for treatment discontinuation?
ActiGraft protocol follows a weekly application schedule, with clinical assessment at each visit determining continuation, frequency adjustment, or step-down to standard dressing management. The standard course is 4–12 weekly applications, with wound area and depth re-assessment at each visit using standardised wound measurement (tracings, digital photography, or 3D wound scanning per EWMA documentation standards). Clinical endpoints for treatment progression: (1) Positive response (continue ActiGraft): ≥30% wound area reduction per 4-week assessment period — consistent with IWGDF/EWMA 4-week response benchmark as predictor of eventual complete closure; (2) Complete healing endpoint: 100% wound closure confirmed at two consecutive weekly assessments with intact epithelialisation; (3) Stepdown to standard care: wound achieving >75% closure, no depth, and advancing epithelial edge can transition to non-adherent standard dressing management without further ActiGraft application; (4) Reassessment for surgical escalation: wounds failing ≥30% area reduction after 4 applications should be reassessed for surgical wound debridement, negative pressure wound therapy (NPWT/VAC), dermal substitute (Integra, Matriderm), or split-thickness skin graft — ActiGraft as a biological therapy augments but does not replace surgical wound management for deep, cavity, or tunnelling wounds. Per the EWMA 2019 Clinical Decision Framework for advanced wound therapies, failure to progress at 4 weeks with ActiGraft triggers reassessment of underlying factors (infection, ischaemia, pressure, nutrition) before continuing or escalating therapy.
Q5: What systemic nutritional and metabolic optimisation supports ActiGraft wound healing response?
Wound healing is metabolically demanding — a chronic non-healing wound of 10 cm² increases resting energy expenditure by 20–30% and protein requirements by 50% above baseline. Nutritional optimisation concurrent with ActiGraft therapy significantly impacts healing velocity. Protein: the EWMA/ESPEN joint position document (2022) recommends 1.25–2.0 g/kg body weight/day protein for patients with chronic wounds — adequate protein intake provides amino acid substrate for collagen synthesis (glycine, proline, hydroxyproline) and wound immune function. Specific amino acids: arginine (3–9 g/day supplemental) is the precursor for nitric oxide synthesis (endothelial wound vasodilation) and collagen proline hydroxylation; glutamine (0.3 g/kg/day) supports wound immune cell energy metabolism. Vitamin C (500–1000 mg/day): collagen cross-linking co-factor; clinical deficiency produces scurvy-pattern wound dehiscence and impaired neutrophil function. Zinc (15–25 mg/day elemental): co-factor for matrix metalloproteinases (wound remodelling) and keratinocyte proliferation; deficiency impairs epithelialisation. For diabetic patients: glycaemic control (target HbA1c <7.5% per IWGDF/ADA DFU management guidelines) is independently associated with wound closure — each 1% HbA1c reduction above target correlates with approximately 20% improvement in DFU healing rate. Offloading: non-removable total contact casting (TCC) — the IWGDF Grade A Level 1 recommendation for neuropathic DFU offloading — is a mandatory co-intervention with ActiGraft to prevent mechanical disruption of the applied autologous clot between treatment sessions.
分享